According to the United Nations Development Programme (UNDP), in 2015 all the UN Member States adopted the Sustainable Development Goals (SDGs), as a collective call for action to end hunger, protect the world and ensure that all people enjoy peace and prosperity by 2030. Sustainable development is important as it saves the national budget, fulfils the need of people, conserves natural resources, helps in the coordination between the natural resources and people, for generations unborn (UNDP, 2015).
Achieving good health for everyone is not an easy task if we all struggle in it; that is why, on January 1st, 2016, 17 Sustainable Development Goals (SDGs) were drawn up by member nations of the United Nations with the aim of achieving them by 2030. The plan was to ‘leave no one behind’ so we’re all winning. These SDGs are intended to address issues that will transform everyone’s future for viable development while achieving good health and well-being for all. (UNDP, 2015)
Nigeria, as a UN member country is a signatory to the SDGs aiming to strengthen the nation’s environment by 2030. Nigeria contributes to almost 25% of Africa’s childhood visual impairment, being the most populous country in Africa. Children aged between 5 and 15 years were visually impaired by uncorrected refractive error in the recent global estimate of visual impairment due to refractive errors, with a prevalence rate of 0.96 % worldwide (Kawuma & Mayeku, 2002). Nigeria’s healthcare system is badly integrated into all strata and has experienced a range of setbacks. The Local government areas (LGAs) are badly served as health facilities with 774 local governments, the staff and resources are insufficient. The SDGs 2030 aims to “leave no one behind”, and we are all working to reduce visual impairment. Information from the Nigeria National Blindness and Visual Impairment Study (IAPB, 2006 – 2007) expressed that 0.6 percent of kids endure visual impairment and poor vision. Cataract, trachoma, inherent glaucoma, and paediatric retinoblastoma, conjunctivitis, and cornea ulceration brought about by eye injury, measles, xerophthalmia, and refractive errors are the main causes of poor vision. Emergency clinic-based investigations uncovered that over 70% of visual impairment in kids is avoidable and that 80% of the conditions are treatable (IAPB, 2018).
Despite its launch in 2005, NHIS covers less than 10 percent of the Nigerian population, leaving the most vulnerable communities at the hands of not accessible health care services. That means social and financial risk protection is not provided to the most vulnerable populations in Nigeria. In other words, over 90% of the Nigerian population is without health insurance coverage (Onwujekwe, Hanson and Uzochukwu, 2012). The quality of health care services delivered is poor and remains a huge source of concern. Most of the PHC facilities that are supposed to meet the health needs of the poor and rural dwellers are in a poor state due to poor budgetary allocation (Abdulraheem et al. 2012).
In Nigeria, not everyone has access to eye care services and the most neglected set of individuals are women, children, and prisoners; thus, making juvenile inmates doubly neglected. Even in places where healthcare is available, it is quite expensive to access, thus proving the inverse care law which states that the availability of good medical care tends to vary inversely with the need for it in the population served (Bulletin of the World Health Organization, 2017).
We see the inverse care law in eye care, with the areas of the world with the highest prevalence of blindness also having the fewest service providers. We also see it within countries where the most socially disadvantaged—commonly poor, rural women—have the least access to eye care and highest rates of visual impairment. The inverse care law is one reason for health gradients that see health vary across populations with social advantage (WHO, 2016). An example is – northern Nigeria, where the prevalence of visual impairment is highest but healthcare is scarce since “the health workforce is concentrated in urban tertiary health care services delivery in the southern part of the country, particularly in Lagos” (WHO GHWA, 2008).
Vulnerable individuals/groups consist of vulnerable people and without sufficient resources or security. Some of the most vulnerable in the under-served population are women, children, the elderly, ill, internally displaced persons, stateless persons, disabled persons, refugees, and individuals who are immunocompromised (WHO, 2002).
Children generally never complain about vision defects. They are generally unaware of their problem or may adjust to their poor vision. They even used to avoid work that required visual concentration for some time. Uncorrected refractive error can cause adverse effects on the learning process and the ability to learn. Blindness caused by refractive error can also have a dramatic personality effect and in career opportunities, along with causing an economic burden to society. Most children with such diseases are obvious and therefore screening helps in early detection and spectacle correction (WHO, 1997).
Refractive error has been given high priority under the National Blindness Control Programme. This took a central part in the global initiative vision 2020, for the reduction of avoidable blindness (WHO, 1997) under which the “My sight My right” programme and more recently the CBM led Comprehensive Child Eye Health in Nigeria (CCEHiN) is running. Refractive error has been a major cause of visual impairment in school children and screening of school children may play an important role in the detection of refractive errors.
Since the prevalence of uncorrected refractive error was also found to be high, students, parents, and teachers, therefore, need to be educated on signs and symptoms of refractive errors so that they can be detected and corrected early. The younger population in the study had a higher referral rate of refractive errors, organic problems, and muscle in balances than the general population (Wong, 1976). For many developing countries around the world, eye care is scarce amongst the offered general healthcare. This is due to the poor economy, the lack of workers in eye care, and ignorance (WHO, 2007).
Juvenile delinquency is misconduct by someone under the age of 18, which would have been a crime if committed by an adult. Juvenile delinquency is one of the societal challenges that every society faces, and its incidence is on the increase. Delinquency can range from stealing, drug addiction, and all forms of mischief. Some inmates of the juvenile system are “offenders,” children that have committed acts that are not adult offences but may get juveniles into trouble with the law. Some crimes include sexual acts, truancy, cigarette smoking, alcohol consumption, running away from home, constant disobedience to figures of authority, waywardness (Williams, 1996).
The study population is Oregun Juvenile Detention Centre, (formerly named Correctional Centre for Boys), provides social and rehabilitative services to juvenile delinquents in Lagos, Nigeria. It was set up to shelter and correct troublesome children.
In the Centre, they are trained on various skills such as tailoring and print works. The children are involved in various sporting activities. There are approximately 100 children and 10 social workers. It should be noted that such confined groups will in general be progressively neglected. Subsequently, the causing blindness issue is higher in these communities (Kawuma, 2000). A prison is an example of a confined/ isolated group of people. These isolated groups tend to be more vulnerable and blindness disorders are more prevalent in those groups than in the general population.
Smith and Stern (1997) stated that: children who grow up in homes marked by lack of warmth and care, whose parents lack good behaviour-management skills, and whose lives are marked by conflict are more likely to be delinquent, while a loving family may protect children even in a very hostile and damaging setting (pp. 383-384). Experiencing childhood in a home that encounters violence can largely affect future conduct. Farrington, Barnes, and Lambert (1996) inspected 400 young men from South London from ages 8 to 46 and found that having a sentenced relative increased the chances of the young men’s future imprisonment. To buttress this point, Farrington et al. (2001) found that having an imprisoned relative had a large role to play the young men’s chances of incarceration in the future. In addition, the data showed that a father’s incarceration had the biggest impact on their children. These analyses demonstrate that early adverse childhood experiences do have a large impact on future life outcomes.
Globally, cataract, uncorrected refractive errors, and glaucoma are the main causes of blindness and their incidence is 33%, 43%, and 2% respectively. There is currently an estimate of around 153 million visually impaired individuals due to uncorrected refractive errors, i.e., visual acuity < 6/18 in the better eye, excluding presbyopia. Globally, uncorrected refractive error is the leading cause of visual loss in children aged 5–15 years (WHO, 1997). The prevalence of myopia (short-sightedness) among children is rising dramatically, especially in urban South-East Asian regions. The most commonly used refractive error correction options are: spectacles, the simplest, cheapest, and most widely used method; contact lenses are not suitable for all patients or environments (WHO, 1997).
An estimated 19 million children worldwide suffer from visual impairment, of which 12 million are due to refractive errors that could easily be corrected. Studies reported a prevalence of the refractive error from 3% to 13.7% (Yared et al., 2012; Al Wadaani et al., 2012; Uzma et al., 2009; Gao et al., 2012; Grzybowski et al., 2020; Robaei et al., 2006).
Refractive error is one of the most common causes of visual impairment globally. It is estimated that around 2.3 billion people worldwide have refractive errors, of which 1.8 billion have access to adequate eye exams and affordable solutions (WHO, 1997). The SDG 2030 strives to leave no one behind; everyone is working on visual disability elimination. Since children are regarded as vulnerable it is safe to say that a juvenile delinquent is doubly vulnerable. According to Resnikoff et al. (2004) and Foster et al. (1998), uncorrected refractive error is responsible for an estimated 18% (8 million people) of global blindness so there’s a need to assess the refractive error status of various groups.
To compare the proportion of children with ocular anomalies and refractive errors between those incarcerated at a juvenile detention Centre and non-incarcerated children. To compare the presenting visual acuity (VA) among Juvenile Detention Centre and non-incarcerated children ages 9-18 years. This research will assess the distribution of ocular anomalies found amongst these neglected groups.
Hypothesis: There is no significant difference between incarcerated and non-incarcerated children in Lagos, Nigeria (have similar patterns). There’s no significant difference in gender, refractive status/ anomalies between both groups.
Study design: Retrospective comparative study
Study Area: Lagos, Nigeria.
Study Population: A total of 76 juvenile delinquents from Oregun Juvenile Detention Centre and 76 randomly selected children drawn from different locations in Lagos state.
Exclusion criteria: All individuals with incomplete screening data were excluded, Staff and social workers of the detention were excluded.
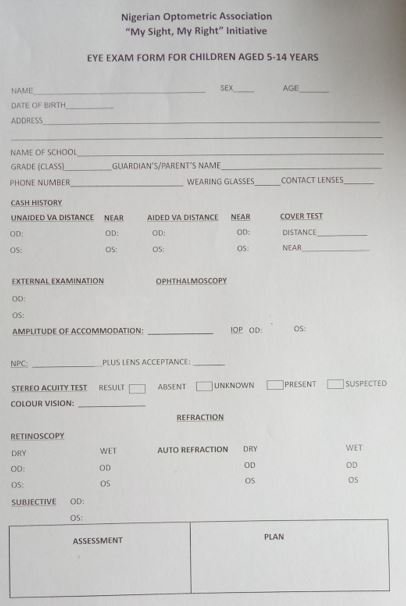
Materials and Methods: With permission from the Nigerian Optometric Association (NOA), data was drawn Nigerian Optometric Association World Sight Day (WSD) 2019 visual screening of juvenile delinquents between age 9-18 and NOA CSR initiative (My sight My right) for children between the ages of 5-14 years. Two randomized groups with the same number of participants were used in study.
Examinations for the World Sight Day (WSD) project included Visual acuity (using the Snellen’s literate and illiterate chart), direct ophthalmoscopy, colour vision test (Ishihara test plates), retinoscopy and subjective refraction while the examination for “My sight My right” which was clinic based, included visual acuity (using the Snellen’s literate and picture chart), direct ophthalmoscopy, colour vision (Ishihara test plates), stereoacuity, non-cycloplegic and cycloplegic refraction by autorefraction, retinoscopy, NPC, A of A.
The juvenile delinquents made up study population; 76 inmates were involved in the study. For the control group, school children under the “My sight My right” programme, were examined, all coexisting eye conditions needing care were identified; refraction was carried out on those needing it, appropriate referrals and medications were issued to those with any form of pathologies.
ETHICAL CONSIDERATIONS: Appropriate correspondence with the head of the detention centre, Oregun, Lagos. Approval was gotten from the NOA to use data for the study. No funding was received in the course of this research work. Statistical methods applied include means, standard deviation, mode, percentages and charts (see appendix).
They are presented in tables (some in appendix) and charts below; The distribution of refractive errors, age, gender, spherical equivalent was available from both groups. Myopia and hyperopia were defined as spherical equivalent of -0.25/+0.25D or worse, astigmatism was defined as cylindrical error >0.25 D and anisometropia as an interocular difference in spherical equivalent powers exceeding 0.50 D. Focusing on the deviations from the norm.
Figure 1: Chart Distribution of ocular morbidities in study: Higher occurrence of refractive errors in control group, higher percentage of pathologies and more referrals in study group.

Among all individuals with refractive errors 1.6% were unilateral and 98.4% were bilateral involvement. On the right eye 24 from the study group and 38 from the control group had refractive errors. On the left eye 23 from the study group and 38 from the control group had refractive errors. Only one person (a 9-year-old) from the study group had unilateral refractive errors. No one from the control group was found with unilateral refractive errors.
A total of 62 persons had refractive error in one or both eyes, giving a prevalence of 38.7% vs 61.3% amongst study and control groups respectively. The commonest single refractive error was astigmatism which accounted for 32.26% (8.06% of incarcerated Vs 24.2% of non-incarcerated) of all errors. This was followed by myopia 29 % (14.5% vs 14.5%) and hypermetropia 27.4% (16.1% vs 11.3%) was the least common.
Most refractive errors occurred among persons aged 14 years at a prevalence of approximately 28% for non-incarcerated.
Table 1: Distribution of ocular morbidities in study: Higher occurrence of refractive errors in control group, higher percentage of pathologies and more referrals in study group.
Diagnosis | Total | Incarcerated | Non incarcerated | |||||
Number | (%) | Number | Males | Females | Number | Males | Females | |
Refractive errors | 58 | (38.2%) | 26 (34%) | 24 | 2 | 34 (44.7%) | 5 | 29 |
Bacterial conjunctivitis | 5 | (3.3%) | 3 (3.9%) | 4 | 0 | 1 (1.3%) | 0 | 1 |
Allergic conjunctivitis | 44 | (29%) | 40 (52.6%) | 37 | 3 | 4 (5.3%) | 1 | 3 |
Glaucoma Suspect | 2 | (1.3%) | 2 (2.63%) | 2 | 0 | 0 | 0 | 0 |
Lens Opacity | 1 | (0.66%) | 1 (1.3%) | 1 | 0 | 0 | 0 | 0 |
Accommodative issues | 4 | (2.6%) | 0 (0) | 0 | 0 | 4 (5.3%) | 0 | 4 |
Low vision | 1 | (0.66%) | 1 (1.3%) | 1 | 0 | 1 (1.3%) | 0 | 1 |
Retinal detachment | 1 | (0.66%) | 1(1.3%) | 1 | 0 | 0 | 0 | 0 |
No Anomalies | 42 | (27.6%) | 9 (11.8%) | 9 | 0 | 33 (43.4%) | 8 | 25 |
Referred Cases | 8 | (5.3%) | 7 (9.2%) | 7 | 0 | 1 (1.3%) | 0 | 1 |
Table 2: Distribution of major ocular morbidities in study: Amongst both groups myopia and hyperopia were equally represented. Astigmatism was relatively high amongst the non – incarcerated group while pathologies were higher in the incarcerated group.
non-incarcerated children | incarcerated children | Total | |
Myopia | 9 | 9 | 18 |
Hyperopia | 8 | 10 | 18 |
Astigmatism | 15 | 5 | 20 |
Low Vision | 0 | 1 | 1 |
Anisometropia | 2 | 0 | 2 |
Accommodative insufficiency/Infacility | 4 | 0 | 4 |
Pathologies | 4 | 49 | 53 |
Several studies have shown that the major cause of visual impairment in the world is an uncorrected refractive error (Naidoo et al., 2007; Dandona & Dandona., 2008). Global figures show that over 2.3 billion people worldwide suffer from reduced vision due to refractive error; 670 million of whom are considered visually impaired because of refractive error (Resnikoff et al., 2008; Thulasiraj et al, 2003).
In Nigeria, several studies have been carried out among different groups of people reporting the common causes of ocular morbidity. Especially in this part of the world, the literature on the prevalence of eye diseases among prisoners is scarce. Ekwenchi, (2001) found a 26.8 percent prevalence of eye disease in his study on the pattern of eye disorders among prisoners in Onitsha Nigerian prison, with ocular conditions such as presbyopia (21.5%), pterygium (19.3 %), refractive errors (25.6 %) and allergic conjunctivitis (12.5 %) observed. One inmate was blind (0.19%) and twelve (1.29%) were blind in one eye only. Five inmates had a poor vision (0.5 %).
Pearce et al, (1972) observed that a relatively high proportion of inmates had not received adequate optometric care prior to that obtained in the prison, in other words, they had received significantly less care than comparably aged males who present themselves to public clinics and private practitioners for routine optometric services.
In a study conducted by Brian et al., (2004) on the incidence and significance of low visual acuity in a prison population around one-third of the inmates had a Visual Acuity (VA) of 6/9 or less in one or both eyes, compared to 11.4% in the control group. There were 24 hyperopes, 14 myopes, and 56 astigmats in the prison category of subnormal Visual Acuity. It is notable that there were five times as many myopias in the control as in the prisoner community in addition to the refractive defects, some 56 prisoners showed ocular disease and other anomalies.
In a study by Muhammad et al., (2019), there were 56.29% individuals who had normal vision (better than 6/12), conjunctivitis was seen in 3%, glaucoma in 1% and cataract in 2% of the individuals, 4.07% Myopia, 3.33% Hyperopia, 2.22% Astigmatism and Presbyopia 34.07%.
Within Nigeria refractive errors in children and adolescents vary from 5.8 % Ilesa east local government area in south western Nigeria (Ajaiyeoba et al., 2006), 6.9% in the study of Ayanniyi et al., (2010), to 79.5 % in other areas within Nigeria – Emerole et al., (2011). In Ethiopia, Refractive errors in either eye were present in (9.4%) of the study group (Yared et al., 2012). Festinger et al., (2004) in their study to assess the vision status among foster children in New York City revealed that refractive error was the most prevalent visual dysfunction, exhibited by 66.7% of children. Vergence dysfunction, shown by 40.8% of the children, was the next most common. Subnormal Visual acuity, was the third most frequent problem, shown by 39.5% of the children. Harrie and Harrie (2016), in their study found out a large percentage of juveniles had uncorrected refractive errors (34.87 %) so also with this study. Naidoo et al., (2007) study revealed that, 6.4 % were visually impaired. 44.5 % had refractive error, 31.2% cataract, 6.0% glaucoma, 4.1% hypertensive retinopathy and 1.4% diabetic retinopathy in contrast to this study were there was no case of hypertensive retinopathy and diabetic retinopathy. Thirty-one participants (0.9 %) were bilaterally blind with the main causes being cataracts (54.8 %) compared with 1.3% in our study.
In the study of Ayanniyi et al., (2010), Two hundred and seventy-seven pupils had ocular pathology giving a prevalence of 19.9%. The two most common ocular disorders observed among the pupils were refractive errors and vernal conjunctivitis with a prevalence of 6.9%, and 6.7% respectively. More than three-quarters (86.7%) of the pupils’ causes of visual impairment and blindness was preventable so also with this study as most issues isolated were preventable.
The age range of both groups was between 9 to 18 years with the mean, for the males’ study group being 15 years and females being 14 years while the control males were 12 years and females 13 years; mode of age was 15 years and 14 years for study and control groups. It is noteworthy that astigmatism is actually lower in the incarcerated group; which contradicts the study by Wong (1976); where the referral rate for astigmatism was higher among inmates than the general population. In Wong’s study refractive error was higher in the study group than among the control group. It can be observed in our study that, most of the study group are males which correlates with several studies that show that more males commit crimes / to carry out delinquent acts than females (Carrabine et al., 2004; Rowe et al., 1995; Walker et al., 2013).
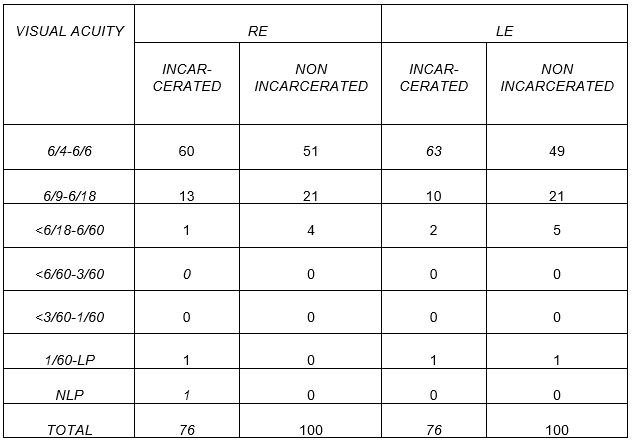
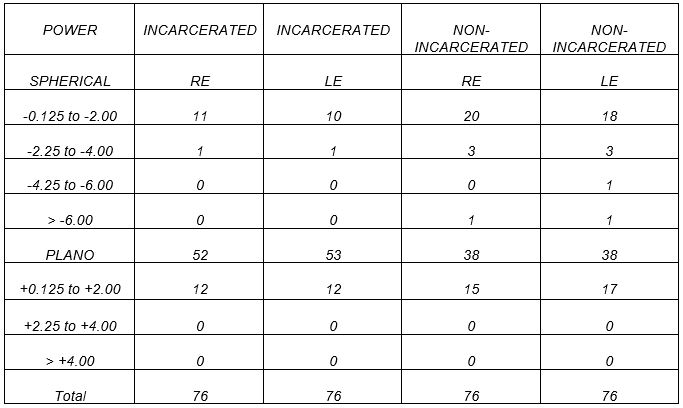
The data for uncorrected refractive errors in this study for the incarcerated group – 34% agrees with the study Harrie and Harrie (2016) 34.7%. Although the data breakdown of refractive errors is different from that of the study. Approximately 70% of the incarcerated individuals and two-thirds of the incarcerated individuals recorded a VA of 6/6 or less in one or both eyes. Interestingly, the study group has more individuals with Plano spherical equivalent than the control group. One individual was blind in the right eye due to retinal detachment and one had severe impairment in both eyes due to lens opacity. Based on this study, a significant number of children from 9 to 18 years (72.4%) have ocular morbidities, being refractive error (38.2%) the major cause of the morbidity, followed by pathologies (34.8%), comprising mainly of allergic conjunctivitis, bacterial conjunctivitis, lens opacity, retinal detachment, and glaucoma suspects, being 29%, 3.3%, 0.66%, 0.66%, and 1.3% respectively. No significant difference in the prevalence of refractive errors in both groups, but a significant difference in pathologies were observed between the groups of the incarcerated and non-incarcerated children. A higher occurrence of refractive error in non-incarcerated children (44.7%) than incarcerated ones (34%); could be attributed to high visual demand due to school work load, prolonged use of digital devices, and screens unlike the incarcerated group with little or no access. The incarcerated group also spends more time on extracurricular activities hence the lower values for refractive errors. Twenty-four children (7 incarcerated; 17 non-incarcerated) had no complaints but were found to have ocular morbidities. Also, observable is that more females had no anomalies in the control group. Morrongiello et al., (1998) deduced that boys could be more likely than girls to participate in a risky activity. This might be the reason behind the incarcerated group having lens opacity and retinal detachment.
Of the 152 children, allergic conjunctivitis is the most common surface disorder in both groups of children, which agrees with several studies (Nwosu, 1999; Adegbehingbe et al., 2005; Bodunde et al., 2004; Akinsola et al., 1993; Ezegwui et al., 2005). Children aged 15 years made up the largest group among the incarcerated. Allergic conjunctivitis (29%) and refractive errors (38.2%) were the most common conditions. The age of 9-18 represents, an adventurous age group, making them more vulnerable. The incarcerated group had more allergic conjunctivitis largely due to a relatively dusty environment which is a risk factor for the development of chronic allergic conjunctivitis.
Some of the limitations of the study include lack of adequate data for the incarcerated group which led to reducing the sample size for the control (non-incarcerated) group; hence the use of random data for the control group. Gender bias in both groups; as most incarcerated individuals are males when compared with the non-incarcerated group which has more females; the percentage of having more males is normal in such institutions. Data was collected by different clinicians in different settings and times. A lack of data on the tribe, other physical challenges, and socioeconomic status.
There is a significant difference between incarcerated and non-incarcerated children in Lagos, Nigeria; as they do not have similar patterns. There’s a significant difference in gender distribution, type of refractive status and ocular surface anomalies between both groups. The study group had more issues that were sight threatening unlike the control group who had more errors.
It would be recommended a provision of health education and periodic visual screening programs for this vulnerable group, which will help in the early detection of refractive errors, and common ocular diseases. The Juvenile detention centers/authorities should allow, or plan with Non-Governmental Organizations (NGOs) or volunteer eye care professionals to offer accessible ophthalmic service for these juvenile delinquents, educate and train social workers to prevent sight-threatening ocular morbidities among vulnerable individuals, thus achieving Universal Health coverage goal. Sight is not just the right of the child; it is the right of everyone even the vulnerable so, there is also a need to properly monitor and evaluate the eyes if we are to “leave no one behind”.
Abdulraheem, I., Olapipo, A., Amodu, M. (2012). “Primary health care services in Nigeria: critical issues and strategies for enhancing the use by the rural communities”, Journal of Public Health and Epidemiology, 4, 5-13.
Abimbola, S., Okoli, U., Olubajo, O., Abdullahi, M., & Pate, M. (2012). The Midwives Service Scheme in Nigeria. Plos Medicine, 9(5), https://doi.org/10.1371/journal.pmed.1001211.
Adegbehingbe, B., Adeoye, A., Onakpoya, O. (2005). Refractive errors in childhood. Nigerian Journal of Surgical Sciences, 15, 19–25.
Ajaiyeoba, A., Isawumi, M., Adeoye, A., Oluleye, T. (2006). Prevalence and Causes of Eye Diseases amongst Students in South-Western Nigeria. Annals of African medicine, 5(4).
Al Wadaani, F., Amin, T., Ali, A., Khan, A. (2012). Prevalence and pattern of refractive errors among primary school children in Al Hassa, Saudi Arabia. Global Journal Health Science, 5(1):125-134. doi:10.5539/gjhs.v5n1p125.
Akinsola, F.B. (1993) Pattern of eye diseases in Nigerian children seen at Lagos University Teaching Hospital. Nigerian Medical Practitioner, 25, 47–53.
Ariel, B.R., & Loran, D.F. (2004). The incidence and significance of low visual acuity in a prison population. Optometry today, Dec 3, 32-34. Retrieved on 20th August 2020 from https://bulger.co.uk/prison/Eye_disease_prison.pdf.
Ayanniyi, A., Mahmoud, A., Olatunji F. (2010). Causes and prevalence of ocular morbidity among primary school children in Ilorin, Nigeria. Nigerian Journal of Clinical Practice, 13(3), 248-253.
Bodunde, O., Onabolu, O. (2004) Childhood eye diseases in Sagamu. Nigerian Journal of Ophthalmology, 12, 6–9.
Carrabine, E., Iganski, P., Lee, M., (2004). Criminology: A Sociological Introduction.
London: Routledge, pp. 88.
Dandona, L., and Dandona, R. (2008) Bulletin World Health Organization. 86(8). Retrieved from https://www.who.int/bulletin/volumes/86/8/08-053652.pdf .
Effective School Eye Health Strategy in Nigeria – IAPB (2020). Retrieved 25 June 2020, from https://www.iapb.org/sib-news/effective-school-eye-health-strategy-in-nigeria/.
Ekwenchi, E. (2001) Pattern of Eye Problems among prisoners in Onitsha prison. Fellowship Dissertation. National Postgraduate Medical College of Nigeria, 17- 27.
Emerole, G., Nneli, R., Anyaehie, U., Okereke, C., Osims, E., (2011) Prevalence, Determinants and Distribution of Refractive Errors in a Nigerian Community. Bioscience Biotech Research Asia, 8(2).
Ezegwui, I., Onwasigwe, E., (2005) Pattern of eye disease in children at Abakaliki, Nigeria. International Journal of Ophthalmology, 5, 1128–30.
Festinger, T., Duckman, R., (2004). Vision status among foster children in NYC: a research note. Social work in health care, 38(4), 77–81. https://doi.org/10.1300/J010v38n04_05.
Foster, A., Gilbert, C., Johnson, G. (2008) Changing patterns in global blindness: 1988-2008. Community Eye Health Journal, 21, 37–39.
Gao, Z., Meng, N., Muecke, J., Chan, W., Piseth, H., Kong, A., Jnguyenphamhh, T., Dehghan, Y., Selva, D., Casson, R., Ang, K. (2012). Refractive error in school children in an urban and rural setting in Cambodia. Ophthalmic epidemiology, 19(1), 16–22. https://doi.org/10.3109/09286586.2011.632703
Grzybowski, A., Kanclerz, P., Tsubota, K., Lanca, C., Saw, M. (2020). A review on the epidemiology of myopia in school children worldwide. BMC Ophthalmology, 20(1), 27. https://doi.org/10.1186/s12886-019-1220-0.
Gilbert, C., Anderton, L., Dandona, L., Foster, A. (1999). Prevalence of visual impairment in children: a review of available data. Ophthalmic epidemiology, 6(1), 73–82. https://doi.org/10.1076/opep.6.1.73.1571.
Global Initiative for the Elimination of Avoidable Blindness. (1997) Geneva, Switzerland: WHO program for the prevention of blindness, World Health Organization, Geneva, Switzerland: World Health Organization, WHO/PBL/9761 9.
Harrie, R.P., Harrie, P.C., (2016) The Prevalence of Uncorrected Refractive Errors in Adolescents Incarcerated in a Youth Detention centre. Child Adolescence Social Work Journal, 33, 273–277. https://doi.org/10.1007/s10560-015-0422-4.
Hatch, S.W. (1990) Visual acuity in the prison population. Optometric Vision Science, 67(5), 382-384.
Iyiade, A., Omotoye, O. (2012). Pattern of eye diseases among welders in a Nigeria community. African Health Sciences, 12(2). https://doi.org/10.4314/ahs.v12i2.21.
Kawuma, M. (2000). Eye diseases and blindness in Adjumani refugee settlement camps, Uganda. East African medical journal, 77(11), 580–582. https://doi.org/10.4314/eamj.v77i11.46724.
Kawuma, M., & Mayeku, R., (2002). A survey of prevalence of refractive errors among children in lower primary schools in Kampala district. African Health Sciences, 2, 69-72.
Moore, M., & Tatman, A. (2016). Adverse Childhood Experiences and Offender Risk to Re-offend in the United States: A Quantitative Examination. International Journal of Criminal Justice Sciences, 11(2), 148–158. Retrieved 17 June 2020 from https://www.sascv.org/ijcj/pdfs/moore&tatmanijcjs2016vol11issu2.pdf.
Morrongiello, B., Rennie, H. (1993) Why Do Boys Engage in More Risk Taking Than Girls? The Role of Attributions, Beliefs, and Risk Appraisals, Journal of Pediatric Psychology, 23(1), 33–43, https://doi.org/10.1093/jpepsy/23.1.33.
Muhammad, I., Javed, A., Hussian, A. (2019) Frequency of Ocular Diseases in the Prisoners of District Jail Lahore. Pakistan Journal of Ophthalmology, 35(4).
Naidoo, K.S., Holden, B., Sweeney, D., Colvin, M. (2007). Design of a blindness prevention reporting and planning tool utilizing the results of a population-based study of visual impairment in a health district in KwaZulu-Natal. Investigative Ophthalmology & Visual Science, 48, 327.
Nwosu, S. N. N. (1999) Childhood eye diseases in Anambra State, Nigeria. Nigeria Journal of Ophthalmology, 7, 34–8.
Onwujekwe, O., Hanson, K., & Uzochukwu, B. (2012). Examining inequities in incidence of catastrophic health expenditures on different healthcare services and health facilities in Nigeria. PloS one, 7(7), e40811. https://doi.org/10.1371/journal.pone.0040811.
Pearce, R. L., Reed, D. R., & Hofstetter, H. W. (1972). Optometric data characteristics of male prison inmates. American journal of optometry and archives of American Academy of Optometry, 49(8), 661–672. https://doi.org/10.1097/00006324-197208000-00006.
Resnikoff, S., Pascolini, D., Etya’ale, D., Kocur, I., Pararajasegaram, R., Pokharel, G. P., Mariotti, S. P. (2004). Global data on visual impairment in the year 2002. Bulletin of the World Health Organization, 82(11), 844–851.
Robaei, D., Kifley, A., Rose, K. A., Mitchell, P. (2006). Refractive error and patterns of spectacle use in 12-year-old Australian children. Ophthalmology, 113(9), 1567–1573. https://doi.org/10.1016/j.ophtha.2006.02.066.
Rowe, D; Vazsonyi, A., Flannery, D., (1995). “Sex Differences in Crime: Do Means and Within-Sex Variation Have Similar Causes?”. Journal of Research in Crime and Delinquency, 32, 84–100. doi:10.1177/0022427895032001004.
Seeing is Believing News – IAPB. IAPB. (2006-2007). Retrieved 12 June 2020, from https://www.iapb.org/sib-news/.
SiB-Monitoring Systems – IAPB. IAPB. (2020). Retrieved 20 June 2020, from https://www.iapb.org/sib-news/seeing-is-believing-nigeria-supports-the-federal-ministry-of-health-national-eye-health-programme-to-develop-eye-health-indicators-and-hmis-tools/.
Smith, C. A., & Stern, S. B. (1997). Delinquency and antisocial behavior: A review of family processes and intervention research. The Social Service Review, 382-420.
Socialprotection.org. 2020. Health Care in Nigeria: Challenges and Recommendations. [online] Available at: <https://socialprotection.org/discover/blog/health-care-nigeria-challenges-and-recommendations> [Accessed 20 June 2020].
Sustainable Development Knowledge Platform. Sustainabledevelopment.un.org. (UNDP 2016). Retrieved 12 June 2020, from https://sustainabledevelopment.un.org/.
Thulasiraj, R., Aravind, S., Pradhan, K. (2003) Spectacles for the Millions Addressing a priority of “VISION 2020 – The Right to Sight” Community Ophthalmology, 3, 19–21.
Uzma, N., Kumar, B. S., Khaja, M. S., B. M., Zafar, M. A., Reddy, V. D. (2009). A comparative clinical survey of the prevalence of refractive errors and eye diseases in urban and rural school children. Canadian journal of ophthalmology, 44(3), 328–333. https://doi.org/10.3129/i09-030.
Walker, J., Maddan, S. (2013). Understanding Statistics for the Social Sciences, Criminal Justice, and Criminology. Burlington: Jones & Bartlett Learning p. 99
Wedner, S., Ross, D., Balira, R., Kaji, L., Foster, A. (2000) Prevalence of eye diseases in primary school children in a rural area of Tanzania. British Journal of Ophthalmology. 84, 1291–7.
WHO | Nigeria. Who.int. (2020). Retrieved 25 June 2020, from https://www.who.int/workforcealliance/countries/nga/en/.
Who.int. 2020. WHO | Vulnerable Groups. [online] Available at: <https://www.who.int/environmental_health_emergencies/vulnerable_groups/en/> [Accessed 20 June 2020].
Williams, Vergil L. (1996) Dictionary of American Penology. Second Edition. Westport, Greenwood Publishing Group, 213.
Wong, S. (1976). Vision Analysis and Refractive Status of Youths in a Juvenile Detention Home Population. Optometry and Vision Science, 53(3), 112-119. https://doi.org/10.1097/00006324-197603000-00003.
Worku, Y., Bayu, S. (2002) Screening for ocular abnormalities and subnormal vision in school children of Butajira town, southern Ethiopia. Ethiopian Journal of Health Development, 16, 165–71.
Yared, A., Belaynew, W., Destaye, S., Ayanaw, T., Zelalem, E. (2012) Prevalence of refractive errors among school children in Gondar town, northwest Ethiopia. Middle East African Journal of Ophthalmology, 19(4), 372-376. doi: 10.4103/0974-9233.102742.
3. Distribution of the Visual Acuity
4. Distribution of the refractive end point.
5. Definitions:
Cataract: is defined as opacity of the lens of the eye.
Glaucoma suspect: Observation of a pale pathologically cupped disc without carrying out other tests to confirm a glaucoma diagnosis.
Refractive error: is any condition in which the visual acuity is less than 6/6 unaided, and then improves with pin hole.
Visual impairment: is visual acuity of < 6/18 – 3/60 in the better eye with best possible correction.
Ocular anomalies: signs and symptoms that deviate from the clinically defined normal such as abnormal appearance, pathologies and impaired vision.
I am profoundly grateful to Raul Perez for your patience and assistance given throughout the course. I am forever indebted to my wonderful parents, AVM and Mrs. J.A. Okosun for their love, financial support, advice and encouragement throughout the period of my course. To my wonderful husband, Mr. Stanley Ohikhuare, my super children: David, Stephanie, Daniel and Stacey thank you for your love, support and understanding. My heartfelt appreciation goes to my super siblings: Violet, Linda, Lorraine, Amenahawon, Omonkhoa and Joyce and cheerleaders (Dr. Mrs. Mercy Ofuya, Dr. Mrs. O.P. Ani, Dr. Mrs. Ologban, Mrs. Ifeoma Eze, Mr. Francis Nwaobodo); for the concern, prayers and support.
Special thanks go to the NIGERIAN OPTOMETRIC ASSOCIATION (NOA National), WOMEN IN OPTOMETRY (WON), NIGERIAN OPTOMETRIC ASSOCIATION LAGOS (NOA LAGOS CHAPTER) and able EXCOs for help rendered and the data used in the project. Finally, Eternity will not be enough to express my gratitude to God Almighty, My Lord and Saviour. All I am and ever hope to be is because of you!





{kind=link}
{kind=link}
{kind=link}
{kind=link}


